
Alopecia: A Comprehensive Patient Guide
1404/05/22

Alopecia refers to hair loss that may occur on the scalp or other body sites, either temporarily or permanently. The condition may result from genetic predisposition, autoimmune disorders, hormonal changes, stress, nutritional deficiencies, infections, medications, and systemic illnesses. Early, accurate diagnosis and evidence‑based treatment are essential to improve outcomes and quality of life.
Hair Biology in Brief
Hair follicles cycle through anagen (growth), catagen (transition), and telogen (rest/shedding). Normally ~85–90% of scalp hairs are in anagen and ~10–15% in telogen; disruption of this balance produces characteristic hair‑loss patterns.
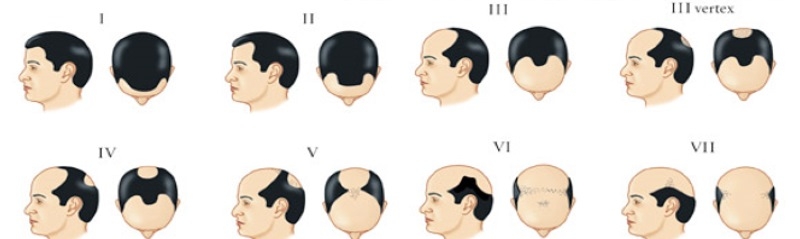
Norwood Scale
The Norwood scale (or Hamilton-Norwood scale) is a commonly used classification system used to measure the extent of male pattern baldness and ranges from stages 1 to 7. It provides easy-to-reference images that indicate different stages of balding.
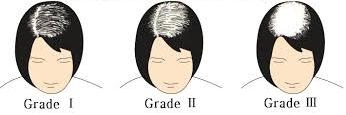
Ludwig Scale
The Ludwig scale is a method of classifying female pattern baldness (Androgenic Alopecia) and ranges from stages 1 to 3.
Major Classes of Alopecia
- Nonscarring (reversible): follicles remain intact (e.g., androgenetic alopecia, alopecia areata, telogen/anagen effluvium, trichotillomania, traction alopecia).
- Scarring/Cicatricial (irreversible): inflammatory destruction with fibrotic replacement (e.g., lichen planopilaris, frontal fibrosing alopecia, CCCA). Therapeutic goal is to halt inflammation and progression.

Nonscarring Alopecias
1) Androgenetic Alopecia (AGA; male/female pattern hair loss)

What is it? The most common hair disorder with polygenic background and androgen sensitivity. Men show frontotemporal/vertex recession; women present with central diffuse thinning.
Diagnosis: History, examination, trichoscopy when needed; selective labs in women with hyperandrogenic signs.
Treatment options:
- Topical minoxidil (2–5%).
- Oral finasteride/dutasteride for selected men (counsel regarding adverse effects); limited, specialist‑guided use in women.
- Low‑level light/laser therapy (LLLT) as an adjunct.
- Microneedling (often combined with minoxidil/PRP) in appropriate candidates.
- Platelet‑rich plasma (PRP) injections as an adjunct to improve hair density/diameter in AGA.
- Hair transplantation in stabilized cases.
2) Alopecia Areata (AA)

What is it? An immune‑mediated, nonscarring alopecia presenting with sudden, smooth patches; may involve brows/lashes and progress to totalis or universalis. Nail pitting and “exclamation‑mark hairs” can be seen.
Therapies:
- Corticosteroids (intralesional/topical; short systemic courses in select cases).
- Topical immunotherapy for extensive/refractory disease.
- JAK inhibitors for moderate‑to‑severe AA in selected adults (with safety monitoring).
- Topical minoxidil as adjunct.
3) Telogen Effluvium (TE)

What is it? Diffuse shedding due to abrupt telogen shift ~2–3 months after triggers such as high fever/infection (including COVID‑19), surgery, childbirth, severe stress, crash dieting, iron deficiency, or thyroid disease.
Course & care: Typically self‑limited and reversible; management focuses on trigger correction, nutritional optimization, stress reduction, and gentle hair care. Evaluate for chronic TE when shedding persists.
4) Anagen Effluvium

What is it? Rapid shedding during anagen, most commonly after chemotherapy or toxins; usually reversible after the insult ends.
5) Trichotillomania & Traction Alopecia

- Trichotillomania: repetitive hair pulling with behavioral/psychiatric underpinnings; managed with CBT and, when indicated, pharmacotherapy.
- Traction alopecia: due to chronic tension hairstyles/extensions; preventable with habit modification and reduced traction.
Scarring (Cicatricial) Alopecias
-Alopecias4.jpg)
- Lichen planopilaris / Frontal fibrosing alopecia: lymphocytic perifollicular inflammation leading to fibrosis; FFA is considered a variant of LPP involving the frontal hairline in women.
- Central centrifugal cicatricial alopecia (CCCA): progressive apical scarring alopecia prevalent in particular populations.
Diagnosis: Trichoscopy may suggest the pattern, but scalp biopsy is the gold standard.
Management (goal: disease control): high‑potency topical/intralesional corticosteroids, calcineurin inhibitors, anti‑inflammatory antibiotics (e.g., doxycycline), hydroxychloroquine, or other immunomodulators per specialist care.
Diagnostic Work‑up at Arian Clinic
- Detailed history (onset, pattern, triggers, medications, diet, stress)
- Examination and trichoscopy
- Targeted labs when indicated (e.g., ferritin, thyroid; vitamin D per clinical context)
- Biopsy for suspected cicatricial alopecia or unclear diagnosis
Treatment Map — At a Glance
-
AGA – Androgenetic Alopecia: Topical minoxidil; oral finasteride/dutasteride (in selected men); low-level light therapy (LLLT); microneedling combined with minoxidil; platelet-rich plasma (PRP) therapy; hair transplantation.
-
AA – Alopecia Areata: Intralesional or topical corticosteroids; topical immunotherapy; JAK inhibitors in selected severe cases; minoxidil as an adjunct treatment.
-
TE – Telogen Effluvium: Address the trigger (e.g., iron deficiency, thyroid disorder, stress); optimize nutrition; stress management; patient reassurance and regular follow-up.
-
Anagen Effluvium: Supportive scalp and skin care; psychosocial support; regrowth typically expected once the causative insult is removed.
-
Cicatricial Alopecias: Anti-inflammatory regimens (high-potency corticosteroids, doxycycline, hydroxychloroquine, others); close disease monitoring.
Supportive Care & Lifestyle
- Stress management and adequate sleep
- Balanced diet with sufficient protein, iron, and micronutrients
- Avoid tight hairstyles and excessive heat styling
- Sun protection for exposed scalp
- Psychological support and patient education
Arian Clinic Services (Shiraz)
- Specialist evaluation and personalized treatment plans
- Medical and injection therapies aligned with current guidelines
- Selected adjunctive procedures (LLLT, PRP, microneedling) for eligible candidates
- Scheduled follow‑ups to track response and optimize care
Conclusion
There is no one‑size‑fits‑all solution for hair loss. Accurate classification, evidence‑based therapy, and regular follow‑up are the keys to optimal outcomes.
References (Selected)
- StatPearls/NCBI — Alopecia (overview): https://www.ncbi.nlm.nih.gov/books/NBK538178/
- StatPearls/NCBI — Androgenetic Alopecia: https://www.ncbi.nlm.nih.gov/books/NBK430924/
- StatPearls/NCBI — Telogen Effluvium: https://www.ncbi.nlm.nih.gov/books/NBK430848/
- AAD — Alopecia Areata: Overview/Treatment: https://www.aad.org/public/diseases/hair-loss/types/alopecia ; https://www.aad.org/public/diseases/hair-loss/types/alopecia/treatment
- PMC — Alopecia Areata: Updated Review (2023): https://pmc.ncbi.nlm.nih.gov/articles/PMC10291119/
- PMC — Pathogenesis/Diagnosis/Therapies of AA (2025): https://pmc.ncbi.nlm.nih.gov/articles/PMC12010142/
- FDA/NAAF — Baricitinib approval for severe AA: https://investor.lilly.com/news-releases/news-release-details/fda-approves-lilly-and-incytes-olumiantr-baricitinib-first-and ; https://www.naaf.org/olumiant-baricitinib-faq/
- PMC — Lichen planopilaris & FFA (2022): https://pmc.ncbi.nlm.nih.gov/articles/PMC9133245/
- PMC — CCCA (2013 & 2025 data): https://pmc.ncbi.nlm.nih.gov/articles/PMC3573455/ ; https://pmc.ncbi.nlm.nih.gov/articles/PMC12047870/
- PMC — PRP for Hair Regrowth (2022 & 2025): https://pmc.ncbi.nlm.nih.gov/articles/PMC8922312/ ; https://pmc.ncbi.nlm.nih.gov/articles/PMC11817460/
- LLLT — Systematic review/meta‑analysis (2021 & 2024): https://pmc.ncbi.nlm.nih.gov/articles/PMC8675345/ ; https://pmc.ncbi.nlm.nih.gov/articles/PMC11023987/
- Microneedling trials/reviews: https://pmc.ncbi.nlm.nih.gov/articles/PMC3746236/ ; https://pmc.ncbi.nlm.nih.gov/articles/PMC8776974/
- COVID‑19 & Telogen Effluvium: https://pmc.ncbi.nlm.nih.gov/articles/PMC9574152/ ; https://pmc.ncbi.nlm.nih.gov/articles/PMC9262270/
- Hair anatomy — StatPearls: https://www.ncbi.nlm.nih.gov/books/NBK513312/
Educational content only; not a substitute for medical care. Please consult a dermatologist for diagnosis and treatment.

User-Comments